

Video Description Title
Video Description description
The information contained in the site is intended for US healthcare professionals only. By selecting “Okay” below, you verify that you are a licensed US healthcare professional.
No
Claudins สามารถพบได้ทั่วร่างกาย แต่มีเพียง 2 isoforms เท่านั้น ที่จะถูกจำกัดอยู่ในเนื้อเยื่อบางประเภท
CLDN18.1
CLDN18.1
เป็น isoform หลัก
ที่พบในเนื้อเยื่อปอด
ทั้งปกติและมะเร็ง
CLDN18.2
CLDN18.2
เป็นisoformหลัก
ที่พบในเนื้อเยื่อกระเพาะอาหารปกติและมักยังคงพบอยู่เมื่อกลายเป็นมะเร็ง
Matteo Fassan, MD, PhD
จำกัดการแสดงออก ในเนื้อเยื่อปกติ
ยังคงมีอยู่และแสดงออกมากขึ้นเมื่อมีการกลายเป็นมะเร็ง
ยังคงอยู่ในระยะแพร่กระจาย


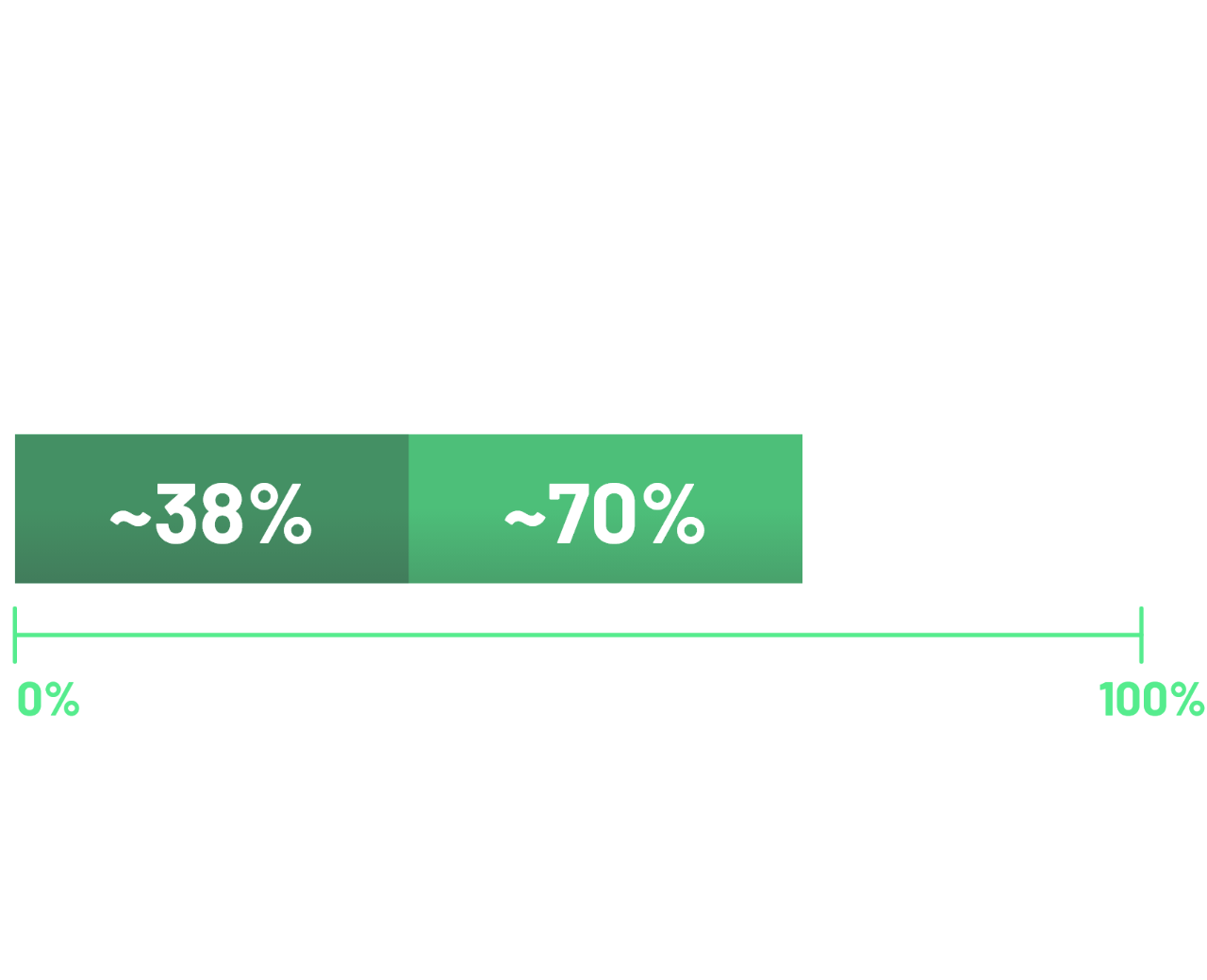
การศึกษาระดับโลก 2 รายงานพบว่า ในกลุ่มผู้ป่วยมะเร็งกระเพาะอาหารและ GEJ ระยะลุกลามที่ไม่สามารถผ่าตัดได้ หรือ ระยะแพร่กระจาย ประมาณ 38% พบการแสดงออกของโปรตีน CLDN18 บริเวณผิวของเซลล์ โดย ≥75% ของเซลล์มะเร็ง มีการติดสีระดับกลางถึงเข้ม (2+/3+)11,12
*For patients diagnosed during 2010-2014.
†Locally advanced (stage II and III) and metastatic (stage IV) G/GEJ cancer per TNM staging classification as described in NCCN Guidelines.19,20
CLDN18.1, claudin 18 isoform 1; CLDN18.2, claudin 18 isoform 2; dMMR, deficient mismatch repair; ESMO, European Society for Medical Oncology; GCs, gastric cancers; GECs, gastroesophageal cancers; G/GEJ, gastric/ gastroesophageal junction; HER2, human epidermal growth factor receptor-2; IHC, immunohistochemistry; PD-L1, programmed death ligand 1; TNM, tumour node metastases.
NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.

ข้อมูลจากผู้ป่วยมะเร็งกระเพาะอาหารและ GEJ พบว่าการแสดงออกของ CLDN18.2 มี high concordance กันระหว่างตัวอย่างที่กระเพาะ (primary) และเซลล์มะเร็งที่ลุกลามไปต่อมน้ำเหลือง9
จากการศึกษาในกลุ่มผู้ป่วยมะเร็งกระเพาะอาหารและ GEJ โดยเป็นชิ้นเนื้อกระเพาะอาหาร (primary)จำนวน 523 ราย และมีการ pair-matched ในกลุ่มผู้ป่วยที่มีการกระจายไปต่อมน้ำเหลืองแล้วอีก 135 ราย9:
เช่นเดียวกับตัวย้อมอื่นๆ เช่น HER2 การแสดงออกของ CLDN18.2 อาจมีความหลากหลายภายในก้อนมะเร็งเดียวกัน ซึ่งควรคำนึงถึงในการเลือกเก็บตัวอย่างในการส่งตรวจ
ในการศึกษาข้างต้น (ที่พบ high concordance ระหว่างเซลล์มะเร็งปฐมภูมิและเซลล์มะเร็งที่ต่อมน้ำเหลือง) พบ intratumoral hetrogeneity ของการแสดงออกของ CLDN18.2 เป็นจำนวน:
ในกลุ่มมะเร็งกระเพาะอาหารชนิดปฐมภูมิ
ในกลุ่มมะเร็งที่ต่อมน้ำเหลือง


References: 1. Pellino A, Brignola S, Riello E, et al. Association of CLDN18 protein expression with clinicopathological features and prognosis in advanced gastric and gastroesophageal junction adenocarcinomas. J Pers Med (Epub) 10-26-2021. 2. Tsukita S, Tanaka H, Tamura A. The claudins: from tight junctions to biological systems. Trends Biochem Sci 2019;44(2):141-52. 3. Hu YJ, Wang YD, Tan FQ, Yang WX. Regulation of paracellular permeability: factors and mechanisms. Mol Biol Rep 2013;40(11):6123-42. 4. ESMO Gastric Cancer Living Guidelines (10-2023). https://www.esmo.org/living-guidelines/esmo-gastric-cancer-living-guideline/diagnosis-pathology-and-molecular-biology/article/diagnosis-pathology-and-molecular-biology. Accessed 01-08-2024. 5. Sahin U, Koslowski M, Dhaene K, et al. Claudin-18 splice variant 2 is a pan-cancer target suitable for therapeutic antibody development. Clin Cancer Res 2008;14(23):7624-34. 6. Niimi T, Nagashima K, Ward JM, et al. Claudin-18, a novel downstream target gene for the T/EBP/NKX2.1 homeodomain transcription factor, encodes lung- and stomach-specific isoforms through alternative splicing. Mol Cell Biol 2001;21(21):7380-90. 7. Sahin U, Schuler M, Richly H, et al. Eur J Cancer 2018;100:17-26. 8. Lamouille S, Xu J, Derynck R. Molecular mechanisms of epithelial-mesenchymal transition. Nat Rev Mol Cell Biol 2014;15(3):178–96. 9. Coati I, Lotz G, Fanelli GN, et al. Claudin-18 expression in oesophagogastric adenocarcinomas: a tissue microarray study of 523 molecularly profiled cases. Br J Cancer 2019;121(3):257-63. 10. Rohde C, Yamaguchi R, Mukhina S, Sahin U, Itoh K, Türeci O. Comparison of claudin 18.2 expression in primary tumors and lymph node metastases in Japanese patients with gastric adenocarcinoma. Jpn J Clin Oncol 2019;49(9):870-6. 11. Shitara K, Lordick F, Bang YJ, et al. Lancet 2023;401(10389):1655-68. Errata in: Lancet 2023;402(10398):290; Lancet 2024;403(10421):30. 12. Shah MA, Shitara K, Ajani JA, et al. Nat Med 2023;29(8):2133-41. 13. Van Cutsem E, Bang YJ, Feng-yi F, et al. HER 2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer 2015;18(3):476-84. 14. Fuchs CS, Ozguroglu M, Bang YJ, et al. Pembrolizumab versus paclitaxel for previously treated PD-L1-positive advanced gastric or gastroesophageal junction cancer: 2-year update of the randomized phase 3 KEYNOTE-061 trial. Gastric Cancer 2022;25:197-206. 15. Abrahao- Machado LF, Scapulatempo-Neto C. HER2 testing in gastric cancer: an update. World J Gastroenterol 2016;22(19):4619-25. 16. Kubota Y, Kawazoe A, Mishima S, et al. Comprehensive clinical and molecular characterization of claudin 18.2 expression in advanced gastric or gastroesophageal junction cancer. ESMO Open (Epub) 01-05-2023. 17. Incidence, survival and mortality for stomach cancer. (2020). In Health at a glance. Asia/Pacific. https://doi.org/10.1787/0c5b2646-en. 18. Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024).Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.who.int/today. Accessed 05-06-2024. 19. National Cancer Institute. SEER Cancer Stat Facts: Stomach Cancer. https://seer.cancer.gov/statfacts/html/stomach.html. Accessed 04-26-2024. 20. American Cancer Society. Cancer Facts & Figures 2024. Accessed March 7, 2024. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2024/2024-cancer-facts-and-figures-acs.pdf. 21. Gress DM, Edge SB, Greene FL, et al. Principles of cancer staging. In: Amin MB, Edge SB, Greene FL, et al, eds. AJCC Cancer Staging Manual. 8th ed. Chicago, IL: American Joint Committee on Cancer, 2017:3-30. 22. Shitara K, Xu R, Moran D, et al. Presented at the 2023 ASCO Annual Meeting; June 2-6, 2023; Chicago, IL, USA. 23. Grillo F, Fassan M, Sarocchi F, et al. HER2 heterogeneity in gastric/gastroesophageal cancers: from benchside to practice. World J Gastroenterol 2016;22(26):5879-87.






